ASU health economist studies effects of mental illness disclosure in the workplace

A person with a serious mental illness must confront the difficult decision of whether to reveal their disorder in their workplace. Disclosing their diagnosis might create stigma, but it could also mean additional support.
Adding to the delicate balancing act is the fact that there’s little information to guide employees toward the right decision.
Marjorie Baldwin, a professor of economics in the W. P. Carey School of Business at Arizona State University, is working on a huge research project to find out how people deal with telling their workplaces about their mental illness and what the outcomes are.
As part of that project, she recently published an article in the journal Psychiatric Services titled, “The Three Cs of Disclosing Serious Mental Illness at Work: Control, Conditions, Costs.”
“I’m a health economist, and for many years, my research has focused on people with disabilities in the labor market,” she said.
“As a result of that research, I became aware that the stigma associated with disabilities is most intense for people with mental disabilities, in general, as opposed to physical disabilities. I began to focus my research on employment outcomes for people with serious mental illness — schizophrenia, bipolar disorder or major depression.”
In 2017, Baldwin was awarded a grant from the National Institutes of Health to collect data and study the topic in greater detail.
Most of the research in this area is on people with serious mental illness who are in supported programs, such as with a job coach, or in a job set aside for a person with a disability. But two problems with supported employment are that the duration typically isn’t long and the wages are usually low.
Baldwin is interested in people with mental illness who find jobs on their own in a competitive labor market and who earn at least minimum wage.
“Those are the jobs that would allow people to be financially independent and not need disability benefits,” she said.
“Many people think that a person with schizophrenia or bipolar disorder would not be capable of working in a competitive labor market, but we’ve talked to hundreds of people doing exactly that.”
Baldwin answered some questions from ASU News:
Question: What are the variables that a person with a mental illness should weigh when deciding to disclose?
Answer: It’s complicated, and that’s why I divided it into three dimensions. The first is control, and that refers to the fact that mental illness in general is concealable. If a person’s symptoms are controlled by medication or their illness is in remission, you wouldn’t know just by looking at them that they have a mental illness.
When disclosing, the big negative that I hear is the fear of stigma. “If I tell them, they’ll look at me differently.”
They weigh the actions they might face if they need job accommodations, like time off for a medical appointment or a flexible schedule, something they’re entitled to under the (Americans with Disabilities Act) but they have to disclose to their employer to qualify for those accommodations.
That is the balancing act.
The second dimension is this idea of the conditions. Disclosure sounds like, “I’ll disclose” or not. But it isn’t a binary choice. There are multiple aspects.
“When will I disclose? Will I wait until after I’m hired, until I get a read of the workplace?”
“To whom will I disclose? Will I tell a co-worker or a supervisor because I need accommodations?”
Most important, “What will I say?” The law mandates that you have to tell your employer about your diagnosis if you want accommodations, but it doesn’t mandate what you have to say.
A lot of people with schizophrenia will say, “I’m not going to say ‘schizo’ anything because there is too much stigma.”
It’s, “I have emotional issues,” or “I have mental health issues.”
The final dimension is cost. “Will I be stigmatized in the workplace? Will people not want to work with me? Will I be passed over for promotion? Will I be fired?” That’s versus the advantages: “I can be the person I really am and I won’t have to pretend. My co-workers might be understanding and helpful. My employer may be willing to give me job accommodations that will let me be more productive.”
There’s no right answer. It depends on personal preference, the conditions in your workplace — whether it’s an accepting culture or less accepting — and your assessment of the benefits and costs.
Q: What are you researching in the project?
A: We just finished four years of collecting data. These illnesses are not rare but they’re not common, so it was difficult to find people in an efficient way.
We piggybacked on a national health survey … They call 7,500 households every month and ask health-related questions. So we added questions to that to find our population.
We talked to 820 people.
This article is the first piece, which lays out the issues of disclosure.
We’re going to analyze the data and look at the aspects that are significantly correlated with whether someone will disclose or not. Our literature review says age may be important — younger people may be more willing to disclose. This is a generation that discloses everything, as opposed to older generations, where people may be more private.
We’ll use econometric models to control for these variables to find out what significant themes emerge around disclosure. And then we’ll link that to employment outcomes.
I’m working with Rebecca White, an associate professor of family and human development in the T. Denny Sanford School of Social and Family Dynamics. We did the surveys of 820 workers, and then for 50 of the workers, we did an intensive, open-ended follow-up interview. We asked them to tell us the stories of their disclosure. That’s qualitative data and takes a different technique to analyze, and she is in charge of that.
People told us what it was like to disclose, why they disclosed and what happened afterward in more detail than we could collect in a half-hour survey.
Q: Why is this research important?
A: We don’t know whether disclosure improves employment outcomes or not.
We want to get this information out to people who have a mental illness as well as to mental health providers.
There’s no data out there for them to say, “These are the situations where it’s a good idea or not.”
Q: Have you studied stigma toward people with mental illness?
A: My previous studies looked at stigma. I worked with a colleague from South Korea, Chung Choe, at Konkuk University. We did a number of papers together, and in the most recent paper we surveyed students at ASU and students at the University of Seoul about stigma toward people with different types of disorders, using a standard scale.
The questions were, “How willing will you be to be a close friend of someone (who uses) a wheelchair,” “Would you be willing to be a co-worker?” “Would you be willing to have them marry into your family?”
The idea of stigma is you want to stay away, you want to avoid them. The way we measure that is what we call “social distance.” And I hate to use the phrase “social distance” because now it means “6 feet.” That’s physical distance, but social distance is how close a relationship you are willing to have with someone.
We asked about 25 disorders of all types.
Previous research with these types of studies typically use mental illness as one category, and they find that mental illness carries a stigma comparable to alcohol abuse, drug abuse and one study included ex-convicts and people with mental illness were right there with ex-convicts.
We wanted to know, is that for all mental disorders or particular ones?
Instead of “mental illness,” we put anxiety disorder, anorexia, schizophrenia, bipolar disorder and major depressive episodes.
And we found that students in Korea and the U.S. in general ranked mental illnesses as more stigmatizing than physical illnesses, and the most stigmatized were schizophrenia and bipolar disorder.
Q: What should people know about colleagues who have mental illness?
A: The stigma associated with mental illness is intense, and it’s driven by stereotypes. We believe everyone with mental illness is characterized by these particular stereotypes, and one of them is incompetence — “They can’t take care of themselves” or “They can’t hold a job.”
That’s just not true.
Some people with acute symptoms will not work and will need support.
But many people whose symptoms are under control or in remission are perfectly capable of living a normal life, holding down a good job and having a family.
That’s an important message to get out there.
For Mental Health Awareness Week, people should be aware that mental illness is an illness. It’s a chemical dysfunction of the brain. It’s not behavior. It’s not something that can be switched off.
Top image by Pixabay
More Health and medicine

ASU team part of nationwide study looking at Type 2 diabetes in youth
Near the end of an interview in which he talked about the work his team will be doing to tackle the rise in Type 2 diabetes among youth, Arizona State University Professor Gabe Shaibi answered why…

Leading the way in wellness: ASU highlighted in The Princeton Review's 2025 Mental Health Services Honor Roll
Being a college student isn’t easy — navigating new routines, people and places can be a challenge, especially if the right support system is not in place. That's why Arizona State University is a…
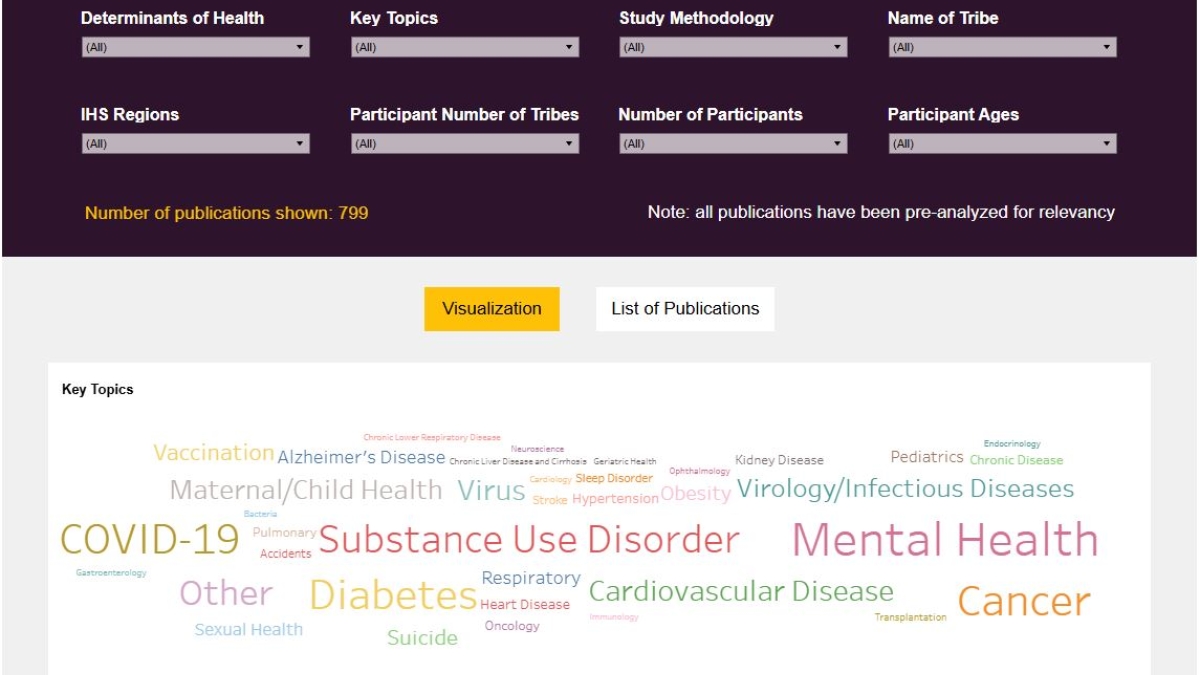
New Indigenous health dashboard offers robust database for scholars
By Nicole Greason and Kimberly Linn A team at Arizona State University’s College of Health Solutions and American Indian Studies program has created a new tool to aid researchers…