
Tragedies like wildfires, floods and mass shootings can’t always be prevented, but the devastating effects can be lessened if hospitals are fully prepared to treat wounded people.
Disaster-preparedness has been a national priority for decades, but efforts were stepped up in the mid-1990s, and, after the 9/11 attacks in 2001, the federal government was spending $500 million a year on various initiatives. One of those was health-care coalitions: partnerships between hospitals and agencies to coordinate disaster response.
Yet lack of coordination remained a major problem during disasters such as Hurricane Katrina and the Las Vegas mass shooting, when some hospitals were overloaded and others had no patients.
Is the government spending worth it? New research by Arizona State University Professor Jonathan Helm finds that not only do health-care coalitions that share information have better patient outcomes, the benefit extends far beyond disasters.
Helm, an assistant professor of supply-chain management in the W. P. Carey School of Business, focuses his research on hospital resources and, with his co-authorsHelm’s co-authors are Alex Mills, Andres Jola-Sanchez, Mohan Tatikonda and Bobby Courtney, all of Indiana University. Their paper was recently posted in the journal Production and Operations Management., created a theoretical model to measure the effectiveness of information sharing among hospitals.

Jonathan Helm
“We came up with some really interesting results that show that the coalitions are significantly more valuable than they thought themselves to be or the government thought they would be," he said. “And it wasn’t the large-scale disasters where they were most valuable, it was the smaller disasters — the three-car pileup on the highway, the bus crash, the small building fire with two to 10 patients.”
Government funding for disaster preparedness doesn’t come with many rules on what the health-care coalitions should do, Helm said.
“It’s fairly nebulous. Some coalitions purchased a lot of supplies and put them in a trailer and said, ‘Here you go, we’re ready for a disaster.’ The problem is that medical supplies are perishable and disasters don’t happen that frequently,” he said.
Helm and his co-authors looked at a coalition founded in 2008 in Indianapolis, which includes 35 hospitals plus emergency and public-safety agencies.
“What they are doing is fairly unique,” he said.
“They created an information-gathering system in which all the hospitals report to the coalition the capacities in their units — in the emergency department, medical-surgical, intensive care, burn beds. They now have a real-time database of all of the medical resources in the city, so instead of stockpiling stuff, they stockpiled information and it updates dynamically.”
Helm emphasized that hospitals are competitors and typically would never share this kind of information.
“They trust the coalition,” he said. “This is information they protect and the creation of this coalition allows them to more freely share it.”
Even for a large hospital, getting more than three patients at one time can be challenging, he said. So when there’s a surge in patients, the coalition can direct where to send them.
“They can distribute the patients across the hospitals in the city. The ones that are less serious they can send a little farther away. The ones that are most serious, they’ll send to this Trauma 1 and when that gets overloaded, they send them to that one.”
The implications can be life-saving.
“If you send a patient to an emergency department that’s overloaded, many things can happen. Morbidity and mortality goes up. Length of stay goes up. Doctors tend to order unnecessary tests because they’re overworked,” he said.
The team created a theoretical model using the variables of incident severity, the capacity at the hospitals and “coordination intensity,” which is how much information is shared. Then they tested it using archived data from the National Trauma Data Bank and hospital census numbers. They found that sharing information on the number of inpatient beds was more valuable than just disclosing how much room is open in the emergency room.
Helm said that proving the credibility of a government-funded initiative was important.
“The question is, given a fixed budget, how do you improve quality?
“We’re having more patients who are able to complete their treatment without being blocked by lack of resources.”
Top photo by Pixabay
More Health and medicine

ASU team part of nationwide study looking at Type 2 diabetes in youth
Near the end of an interview in which he talked about the work his team will be doing to tackle the rise in Type 2 diabetes among youth, Arizona State University Professor Gabe Shaibi answered why…

Leading the way in wellness: ASU highlighted in The Princeton Review's 2025 Mental Health Services Honor Roll
Being a college student isn’t easy — navigating new routines, people and places can be a challenge, especially if the right support system is not in place. That's why Arizona State University is a…
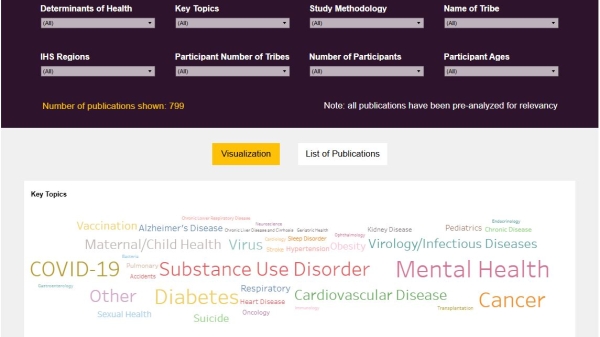
New Indigenous health dashboard offers robust database for scholars
By Nicole Greason and Kimberly Linn A team at Arizona State University’s College of Health Solutions and American Indian Studies program has created a new tool to aid researchers…